Recently, the Tasmanian Government released a draft of the Strategy for public consultation. Four teams from across the University of Tasmania contributed submissions, drawing on expertise in public health, policy and medical research, and workforce development. The submissions strongly endorse the aims of the Strategy and identify key areas where the University could contribute to its design and delivery.
This week’s PIMBY outlines the case for preventive health and what a best practice strategy would look like in Tasmania. We start with an overview of the current health system, before turning to the draft Strategy and drawing on insights from the University’s submissions to highlight what it will take to make the ‘health revolution’ a reality.
Tasmania's health system challenges
The profound challenges facing Tasmania’s health system are well known. Tasmanian Government health spending increased by 59% in real terms between 2015 and 2024, and health’s share of total state spending jumped from 29.9% to 38.5% (see chart below). Despite this investment, the health system continues to struggle to meet demand.

As of December 2025, nearly 71,000 outpatients were on waiting lists, and only
55% of elective surgery patients were seen within the clinically recommended time. Across the state’s emergency departments, only 46% patients were seen on time – well below the
national average of 67%.
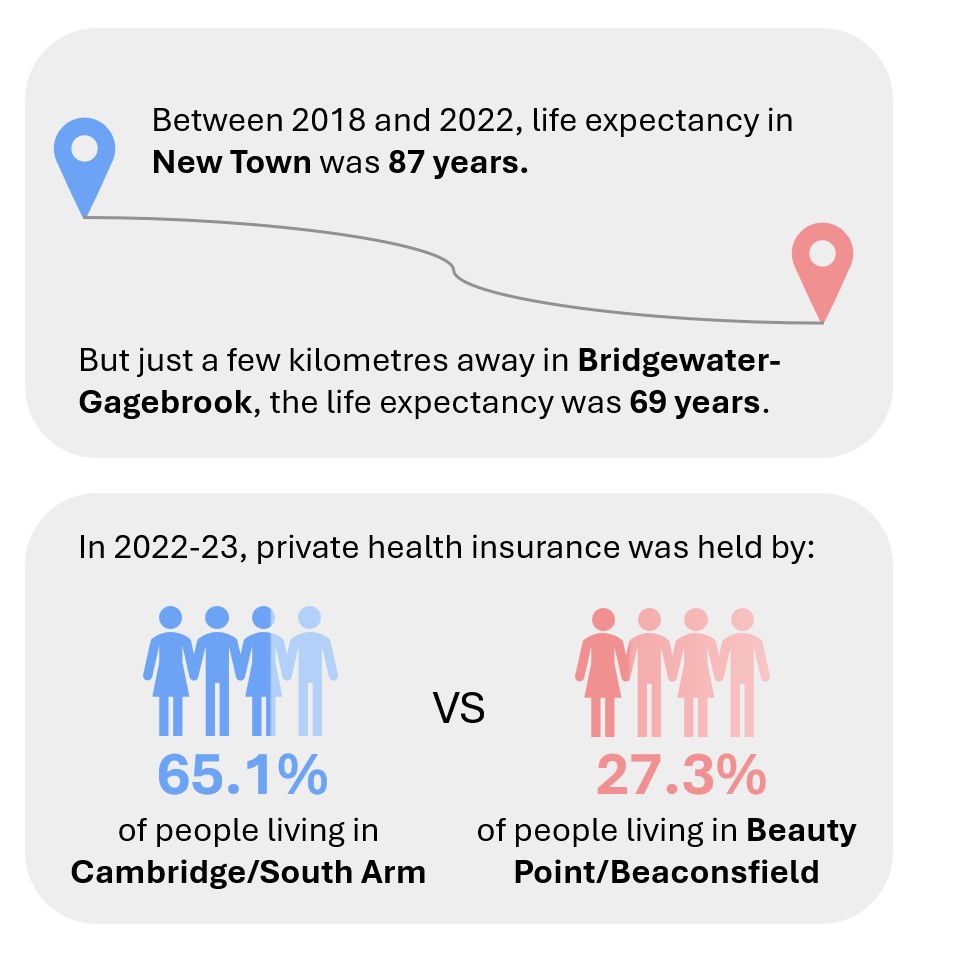
Less obvious (but just as important) is ongoing health inequity. On average, Tasmanians from lower socioeconomic backgrounds or in remote and regional communities experience a higher ‘disease burden’ and barriers to accessing health care and services. The
national Social Health Atlas gives us two examples:
As
Primary Health Tasmania notes (and covered in an
earlier PIMBY), out-of-pocket costs continue to be a key driver of unequal access to care, particularly for people living with chronic conditions, those without concession cards, and residents of rural and remote communities.
With rising costs, increasing demand, and persistent inequity, there is a need for ambitious and innovative reform. In this context,
The Health Revolution (‘the Strategy’) is a timely opportunity to shift the focus from not just treating health problems, but also preventing them.
The Health Revolution
The draft Strategy’s vision recognises that improving health outcomes requires addressing the broader social, economic, and environmental factors that shape people’s health:
Our vision for Tasmania is one of opportunity and fairness - a place where every Tasmanian can live well -through environments that make healthy choices easier, communities that are safe and connected and supports that help people stay well for longer.
The intent is to reduce demand on acute health services by addressing the root causes of poor health. To this end, the Strategy is built around five pillars:

Once finalised, the Strategy will act as an overarching framework to align existing initiatives and guide future work across multiple sectors. It will be implemented through a series of four‑year action plans, the first of which is scheduled to begin in mid‑2026.
In response to the draft, the University of Tasmania made four submissions, each reflecting different areas of expertise.
- University of Tasmania Health – focuses on the need for the Strategy’s ambition to be translated into clear priorities, measurable targets, and a strong evaluation framework. Tasmania’s unique context and health inequities (like chronic health conditions and workforce issues) will need to be recognised.
- Menzies Institute for Medical Research – calls for a coherent and actionable strategy with clear goals, strong use of data and evidence, and alignment between the Strategy’s vision and how it will be implemented.
- Tasmanian Policy Exchange – makes the case for long-term investment in prevention and argues that delivering the Strategy effectively will require new funding models and governance approaches.
- Wicking Dementia Research and Education Centre – identifies dementia prevention as a major priority for Tasmania, where Australia's oldest and most rapidly ageing population faces significant prevalence of dementia risk factors and calls for targeted action across all pillars and stronger alignment with national dementia strategies.
Overall, these submissions point to a common challenge: how to translate a strong vision for preventive health into sustained investment, action, and impact. They also show how the University’s teaching and research can support the implementation of Tasmania’s prevention agenda.
Prevention is better than a cure
One of the most effective ways to improve health outcomes and equity while reducing long-term costs is by investing in prevention. The Productivity Commission
recently found that a $1.5 billion national investment in prevention over five years could deliver governments $2.7 billion in direct savings, plus a further $2.7 billion in broader health, social, and economic benefits. This means that Tasmania could achieve both savings and wellbeing benefits in the future if we invest in high quality, evidence-based prevention now. Which is why it’s confusing that governments across the world almost always consistently underinvest in preventive health.
The Productivity Commission suggested a few key reasons for this:
- Split incentives and responsibility across government: The costs of prevention are often borne by one department, while the responsibilities and benefits are realised across many. In a competitive budget environment, this means departments have less incentive to fund and act on prevention.
- Short-term thinking: Preventive health offers benefits over long periods of time (often beyond electoral and budget cycles) making it less appealing than acute care, which is highly visible and responds to immediate needs.
- Budgeting rules: Current budgeting rules don’t adequately capture long-term and/or cross-portfolio savings, meaning preventive initiatives are often undervalued.
- Challenges in demonstrating impact: Long timeframes, limited data, and scarce evaluation resources make it harder to build the evidence base needed to set priorities and sustain funding.
So, clearly there are reasons why we don’t invest enough in prevention. That said, these barriers can be overcome by strengthening the evidence base for the economic and social benefits of preventive care. And it’s not like Australia is leading the way in this area. In 2023, at least 20 OECD countries allocated a higher share of their health budgets to prevention than us:

Funding the future
Realising the benefits of prevention, especially the savings mentioned earlier, depends on
getting governance and funding settings right. This is key for making sure the Strategy is both successful and sustainable.
Tassie can learn from innovative models such as Victoria’s cross-agency
Early Intervention Investment Fund (EIIF). The EIIF is administered by the Victorian Treasury and fully embedded in the state budget process. Under this model, agencies that deliver prevention projects approved by EIIF receive 50% of anticipated savings up front, with the remainder disbursed as savings are realised. This approach helps address some of the budget and alignment challenges we talked about above. Since its introduction, the Victorian Government has invested $2.7 billion through the EIIF, with more than $3 billion in economic and financial benefits anticipated. The 2024-25 Budget alone committed $1.1 billion to early intervention initiatives.
At the national level, the Productivity Commission’s
Delivering Quality Care report is also important. It proposes a ‘Future Avoided Costs’ (FAC) model similar to the EIIF approach, aimed at investing in evidence-based and value-for-money prevention and early intervention.
The TPE suggested that one good option is to establish a dedicated, centrally-managed preventive health funding pool based on the Victorian EIFF and developed in partnership with the Commonwealth to leverage the proposed national FAC model. We even came up with a cool name: ‘Strategic Health Investment Fund Tasmania’, or SHIFT! This model would also be useful for delivering the Government’s commitments under the 2025
Wellbeing Framework.
The right people with the right skills
Under the Health Systems and Supports pillar, the Strategy appropriately recognises that a "strong, skilled prevention workforce" is essential. However, the preventive health workforce isn’t just a part of the system – it arguably forms its foundation. On top of that, specialist preventive health workforce development is needed to build skills, strengthen communities, and help reduce inequality. Therefore, it should be prominent across all the Strategy’s pillars rather than confined to just one.
Of course, workforce development on its own isn’t enough to drive a health revolution. Preventive health also depends on community capability. While a prevention-focussed system with a highly capable workforce is indeed essential, true preventive health requires environments that enable people to have the knowledge, confidence, and support that enable healthy lifestyles.
Over the Strategy’s 20-year timeline, much of Tasmania’s current workforce will turn over. This gives us an extraordinary opportunity to embed preventive-focused skills, population health thinking, and community-oriented practice across both health and non-health sectors. The University of Tasmania is uniquely placed to support this agenda given its central role in training our future health and care workforce. Alongside this, we can do a lot for community capability by empowering our communities to design and deliver services and initiatives that support preventive health.
For this reason, it’s important that workforce development and community capability are explicitly recognised as cross-cutting enablers in the Strategy, which will shape how all pillars are delivered in practice.
The revolutionary end goal

The Strategy sets out an aspirational vision for a health revolution, but meaningful change will be challenging given the complexity of the health system and limited resources. Meaning, it will be very important for the Strategy to set clear priorities that guide decisions about where to devote effort and funding. Although the current ‘areas of focus’ are useful, the principles that frame the Strategy are quite broad. It’s difficult to see how priorities will be determined or how progress will be tracked over time.
The Strategy also sets out a series of compelling goals – from “every Tasmanian lives in a place that’s safe and healthy” through to “Tasmania has the healthiest population in the country.” But, again, these aren’t supported by clear, quantitative targets, which will be critical for tracking progress and ensuring accountability.
The Strategy’s proposed evaluation and learning framework will be critical. Developing this framework as a priority in the first Action Plan will be important to make sure the work is anchored in measurable outcomes right from the start. If this doesn’t happen, there’s a risk that the work of the Strategy will remain conceptual rather than actionable.
The University is well placed to support this work in several different ways, including developing baseline data, producing locally relevant evidence to inform prevention efforts, and helping to design a robust evaluation approach.
Time for a step change
The University recently made a long-term commitment as part of its 2025
Strategic Plan Refresh to work with partners on improving health outcomes inTasmania. The goal we are working towards is that Tasmania’s average life expectancy at birth exceeds the national average by 2050. In light of this, the University strongly supports the objectives of the Strategy. We’re looking forward to partnering with the state government, health and care-system stakeholders, and wider community to deliver better preventive care for all Tasmanians.
The success and sustainability of the Health Revolution agenda will depend on commitment across government and the Tasmanian community, backed by high quality evidence and an innovative approach to funding and governance. This is an exciting opportunity to establish an ambitious prevention strategy that can deliver a step change in our state’s health system and improve the future health and wellbeing of all Tasmanians.
.png)





.png)



